





During the consultation, the Commission heard repeatedly about ageism and its effects. Ageism can give rise to individual acts of discrimination, but can also have an impact on a wider scale by influencing policies, programs and legislation that affect broad sectors of society. For the purposes of this Report, the term ‘ageism’ refers to two types of behaviour that have a negative effect on older persons. The first involves the social construction of age, including incorrect assumptions and stereotypes about older persons. Another form of ageism involves a tendency to structure society based on an assumption that everyone is young, thereby failing to respond appropriately to the real needs of older persons.
Negative Attitudes and Stereotypes
The consultation emphasized that many barriers faced by older persons are attitudinal. Much of what we associate with aging is simply ‘socially constructed’. In other words, it is not a real component of aging, but rather society’s response to the process.
...the physical side of aging accounts for perhaps 25 percent of aging that we see in American society. Seventy-five per cent is accounted for by another type of aging which has no physical basis. It is the role which our folklore, prejudices, and misconceptions about age impose on “the old”.[2]
The Commission heard many examples of negative attitudes and stereotypes:
“...I was terminated after 24+ years of service at age 58 and was told that “anyone over 50 was unable to be trained.”
“There is a myth that at age 65 people suddenly become ill, demented, dependent and fold their hands and go on the dole.”
(Canadian Pensioners Concerned)“...there is a growing tendency to blame the elderly for... escalating health care costs and difficulties in accessing...services...[This] is often evident in how both the public and media frame discussions of health care issues... [There is a] pejorative labelling of older adults as ‘bed blockers’...” (Ontario Association of Social Workers)
“Stereotyping and negative attitudes... is the dominant theme that we see in the course of our work. We strongly agree that stereotypes about aging and ability of older persons give rise to discriminatory treatment.” (Advocacy Centre for the Elderly)
Perhaps one of the clearest examples of ageism is observed in the Code itself. The definition of age in section 10(1) states:
The restricted definition of age in human rights law, which allows employers to implement mandatory retirement at age 65, demonstrates how deeply ageism is ingrained in our culture.
“age” means an age that is eighteen years or more, except in subsection 5(1) where “age” means an age that is eighteen years or more and less than sixty-five years;
Section 5(1) prohibits discrimination in employment. This means that persons over the age of 65 cannot make a complaint of age discrimination in employment. This also allows employers to implement mandatory retirement at age 65 and prevents anyone from making a complaint that being forced to retire at 65 is discriminatory.
This restricted definition of age in the Code demonstrates how deeply ageism is ingrained in our culture. Some have noted that it also serves to perpetuate ageism as it sends a message that workers over 65 do not have the right to be free from age-based discrimination.
Ageism and its effects extend well beyond the issue of mandatory retirement. The Commission also heard that ageism contributes to elder abuse and plays a prominent role in the barriers to housing, health care, services and institutions. Consultees told the Commission that ageist assumptions can be found in the manner in which health care and service providers approach older persons and the way in which housing options are formulated for older persons in Ontario. In effect, ageism, in its various forms, serves to disempower older persons within these very important aspects of their lives.
Failing to Take the Needs of Older Ontarians Into Account
The Commission heard many examples of the second form of ageism, namely the failure to respond to the real needs of older persons and to design systems and services that are inclusive for older persons:
“Ageist attitudes persist with many physicians, e.g. “what do you expect for your age?” ...especially if there is a mental health problem.” (Canadian Mental Health Association – Windsor-Essex Branch)
- treating certain conditions such as hearing loss or depression as a ‘normal’ part of the aging process and, therefore, not providing appropriate assessment and treatment;
- timing traffic lights based on how long it would take a young person who has no disability to cross the street, instead of taking into account how long it might take an older person, especially someone with a disability, to safely make the crossing;
- focusing health care spending on acute care with insufficient emphasis on long-term, chronic care; and
- providing services with an emphasis on how quickly and ‘efficiently’ people can be served which may result in insufficient time being spent with older clients.
Our society should be structured and designed for inclusiveness. The needs of all citizens, including older persons, must be taken into account up-front so that physical, attitudinal and systemic barriers are not created. Assuming that everyone is young and able-bodied and designing programs and facilities on that basis is a form of ageism that must be addressed in our society. The Commission heard that some levels of government are now undertaking gender-based analysis. Similarly, government should consider the impact of laws, policies and programs on all age groups.
Measures to Combat Ageism
Acknowledging Contributions[3]
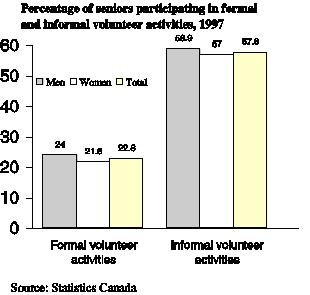
The Commission was told that more emphasis must be placed on the contributions made by older persons. They provide wisdom and experience, as illustrated by the fact that many judges and politicians are older persons, and many are entrepreneurs and employers. Older persons are consumers in the economy and investors; they also play a critical role as caregivers and volunteers. These contributions should be acknowledged through more positive portrayals of older persons.
As one group noted: “Consideration should also be given to the recognition of the part older persons can continue to play, not only as workers, volunteers and citizens...with a wealth of life experience, but also in the development of public policies which affect all people in communities” (Canadian Pensioners Concerned).
Public Awareness Campaigns and the Media
Participants told the Commission that there is a need for public awareness campaigns, using radio, television, print media and other means such as transit ads, to counteract myths and stereotypes about older persons. These campaigns should provide a positive portrayal of older persons by showing them as active and contributing to society. One group noted that these campaigns are not just to combat ageism but also to empower those experiencing ageism to recognize what it is and how to respond. In addition to using the media to raise awareness, it was suggested that there should be monitoring of the portrayal of older persons in the media to ensure that it is balanced and not contributing to negative attitudes.
Initiatives in the Education System
Participants stressed the importance of changing attitudes about older persons at an early age. As one group noted: “Attitudes are established at a young age. Negative images of older persons can generate a strong age bias early in life. Myths and stereotypes are developed. If left unchallenged, they become lifelong beliefs and ageism emerges” (United Generations Ontario).
“Our experience clearly shows that programs and activities that bring members of different generations together in meaningful ways breakdown stereotypes, destroy myths and create a climate of mutual caring and sharing.”
(United Generations Ontario)
Therefore, initiatives to raise awareness about ageism, in both its forms, and the aging process should be introduced into public and secondary schools. One group suggested that intergenerational programs can be particularly successful in breaking down barriers between the generations and combating ageism. An intergenerational program is a planned, intentional interaction of different age groups, infant to elderly, in a variety of situations at a level that provides close communication, sharing of feelings and ideas, and cooperative activity in meaningful tasks. Such programs can serve to promote health and well being not only for older persons but also for society as a whole.[4]
Many of the submissions focused on the need for educational initiatives in post-secondary education and in training for specific jobs. In particular, those who work with the public should receive training that dispels negative assumptions and attitudes and serves to increase awareness of how to appropriately respond to the aging process. Educational initiatives should include enhanced training in gerontology, care-giving skills, communications techniques and education with respect to cognitive deterioration caused by dementias (e.g., Alzheimer Disease). The Commission heard that improved training for doctors, nurses, other health care professionals, police, lawyers, journalists, social workers, policy-makers and others who work directly with older persons would be a starting point:
“The training of [public transit] employees should include age and disability awareness.” (Ontario Coalition of Senior Citizen’s Organizations)
“Special training needs to be provided to caregivers and to those who work in residential complexes for seniors.”
(Canadian Hearing Society)“With the aging of the population and longer life expectancies, physicians need to become more familiar with the aging process and the health needs of older adults. Currently, the five medical schools in Ontario allocate a minimal percentage of their medical school curriculum to aging or dementia...Since family physicians are often the first point of entry into the health care system, it is important that they receive more in-depth training than is currently offered.” (Alzheimer Society of Ontario)
Consultees told the Commission that education must also be aimed at older persons so that they can identify if and when they are experiencing ageism or age discrimination and know what recourses are available to address it.
Additional Measures
Other suggested measures include:
- ongoing communication with the public, especially seniors groups, to identify and discuss ageism and how to combat it;
- province-wide distribution of educational materials on ageism and age discrimination, preferably in written and audiovisual formats;
- public education forums across the province;
- education on ageism in the workplace; and
- the review of all government laws, policies and programs using an “older age analysis” to see if they appropriately take the needs of older Ontarians into consideration.
The Commission is very concerned that ageism and age discrimination do not appear to invoke the same sense of moral outrage and condemnation as other forms of unequal treatment. Recognizing that ageism is ingrained in societal structures and attitudes and that it gives rise to discrimination against older adults the Commission recommends the following specific measures to combat both forms of ageism.
Recommendations for Government & Community Action
2. THAT all levels of government evaluate laws, policies and programs to ensure that they do not contain age-based assumptions and stereotypes and that they reflect the needs of older persons.
3. THAT the Ministry of Education, school boards and schools develop programs and activities that will encourage a better understanding and a more positive perception of older persons. Intergenerational programming between students and older persons is an integral part of such education.
4. THAT professional faculties such as medicine, nursing, social work and nutritional sciences should better prepare their graduates to work with older persons in a more supportive manner, without stereotypes and assumptions.
5. THAT regulated professions and voluntary professional associations take steps to raise awareness among their membership about ageism and age discrimination and provide continuing education in this area, for example through courses and publications.
2. Commission Commitments
1. The Commission will develop a public policy statement on age discrimination in 2001/2002.
2. The Commission will develop and implement a broad public awareness campaign that addresses ageism and age discrimination.
[2] A. Comfort, “Age Prejudice in America.” (1976) 7 Social Policy at 4 as cited in Dr. M. Shipman, “Intergenerational Programming from Instrumental Action to Social Imperative and a Vision of a Civic Society” (Research Commissioned by the Vanier Institute of the Family, August 1996) at 6.
[3] Percentage of Seniors Participating in Formal and Informal Volunteer Activities, 1997 from Health Canada, Division of Aging and Seniors, Statistical Snapshot No. 20: Giving Back to the Community, online: Health Canada, Division of Aging and Seniors <www.hc-sc.gc.ca/seniors-aines/pubs/factoids/en/factoid.htm>.
[4] For detailed information about intergenerational programming, see Shipman, supra, note 2.